
Extraction-to-implant planning
Immediate Implant Placement
Immediate implant placement for selected extraction sites where anatomy, infection control, bone support and soft tissue conditions allow a safe implant strategy.
Extraction-to-implant planning
Surgery is designed before the surgical appointment begins.
Designed for
Non-restorable teeth in suitable extraction sockets
Aesthetic-zone cases requiring careful soft tissue preservation
Patients needing implant planning before extraction
Selected cases where primary implant stability is achievable
Planning records
CBCT assessment of socket walls and root anatomy
Evaluation of infection, bone defects and soft tissue phenotype
Prosthetic position planning before extraction
Decision on immediate, early or delayed implant placement
Clinical sequence
How this treatment is approached.
Diagnosis
A tooth that cannot be saved may sometimes be replaced with an implant at the same surgical visit, but only if the anatomy and risk profile are suitable.
Surgical approach
Atraumatic extraction and socket evaluation Implant placement guided by prosthetic and biological goals Bone grafting or contour augmentation when indicated Provisionalization only when risk profile and stability allow
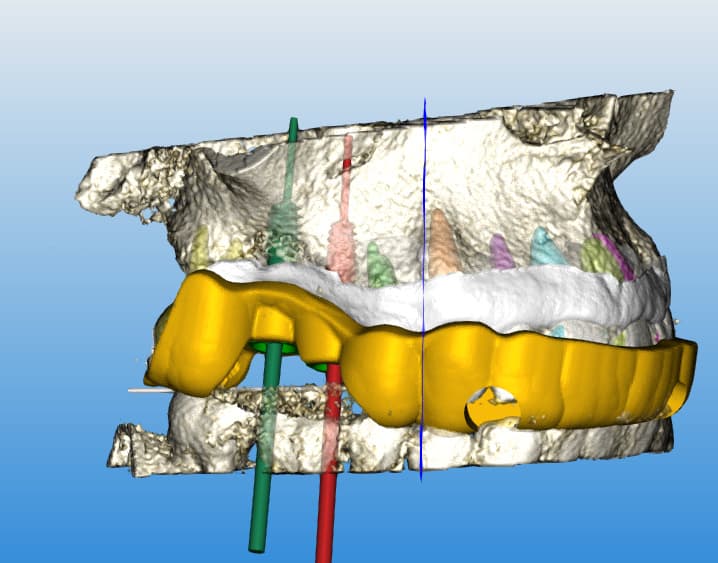
Digital advantage
Digital planning helps decide whether immediate placement is appropriate Guides may support implant positioning in selected cases Pre-surgical visualization can help international patients understand the sequence
Technology and materials
Premium implant systems including Straumann when clinically indicated Socket grafting and contour biomaterials when needed Digital guide splints and provisional planning for selected cases
Digital workflow value
Digital planning helps decide whether immediate placement is appropriate
Guides may support implant positioning in selected cases
Pre-surgical visualization can help international patients understand the sequence
Materials and technology
Premium implant systems including Straumann when clinically indicated
Socket grafting and contour biomaterials when needed
Digital guide splints and provisional planning for selected cases
Important limitations
Precision requires honesty.
Premium surgical planning improves clarity, but treatment suitability and outcome depend on diagnosis, anatomy, tissue quality, healing response and clinical execution.
Limitations to respect
Immediate implant placement is not appropriate for every extraction site
Active infection, missing socket walls or poor stability may require staged treatment
Aesthetic-zone cases require careful risk evaluation before committing to immediacy
Patient pathway
Send X-rays, CBCT and photos of the tooth if available
Clarify whether the tooth is painful, infected or previously treated
Receive guidance on whether immediate or staged implant planning is more appropriate
Clinical information and outcome notice
The information on this website is educational and does not replace an individual diagnosis, clinical examination, radiographic assessment, periodontal charting, CBCT review, or personalised medical advice. Treatment suitability and outcomes vary according to anatomy, health status, diagnosis, healing response, compliance, and other clinical factors.
Related treatment planning
Complex cases often combine several disciplines.
Digital implant planning
Guided implants
A digitally planned implant workflow using clinical records, CBCT information, intraoral scans and guide design to support accurate implant positioning when guided surgery is clinically indicated.
Explore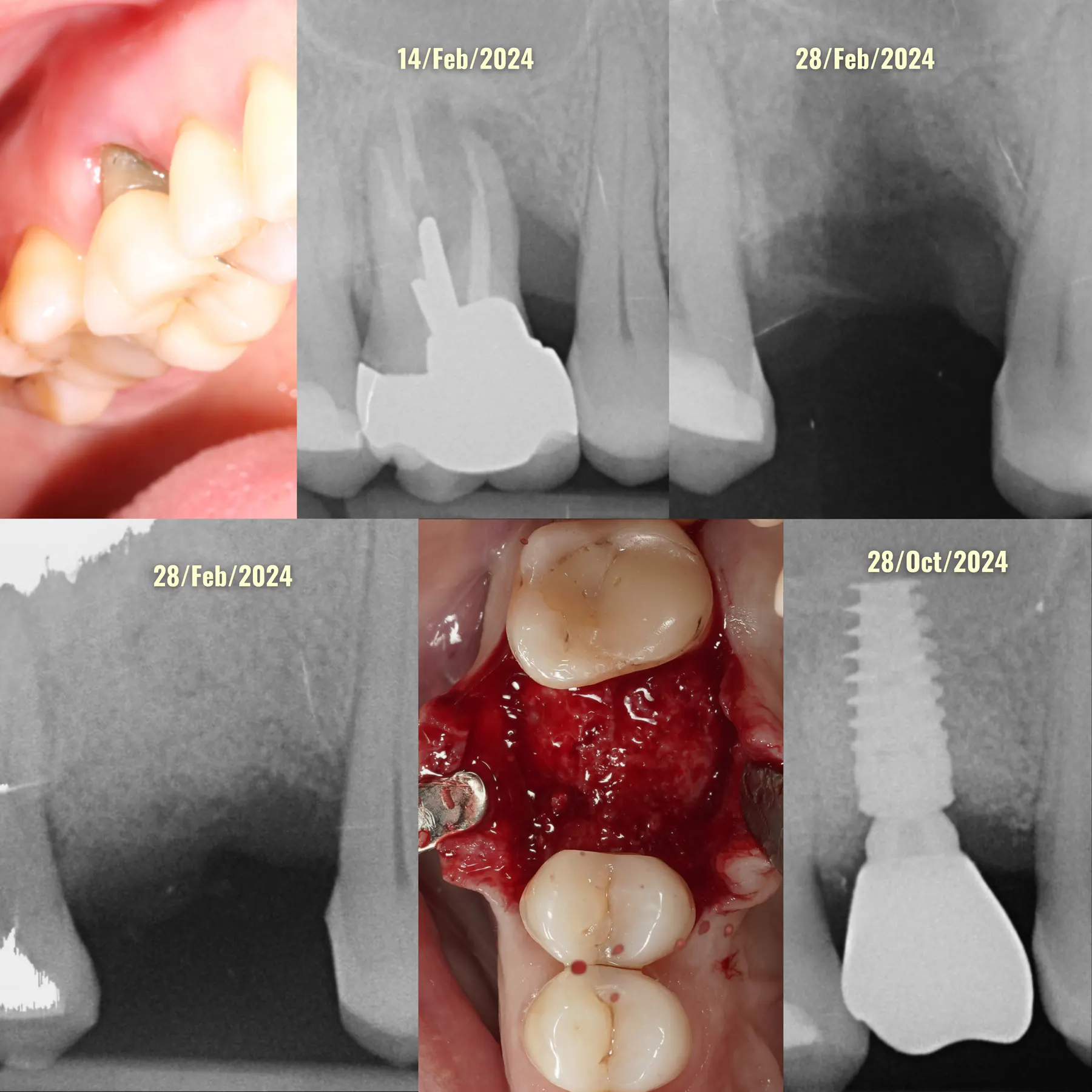
Extraction site planning
Ridge preservation
Extraction-site preservation and implant site development designed to reduce bone collapse and prepare a more stable foundation for future implant placement.
Explore
Tissue architecture
Soft tissue grafting
Soft tissue grafting to improve tissue thickness, keratinized tissue, peri-implant stability and aesthetic tissue architecture around teeth or implants.
ExplorePrivate case review
Send your records before planning treatment.
The first step is to understand your anatomy, diagnosis, expectations and travel context before defining a surgical sequence.